
CT scan generated with a Canon CT to
plan a TAVR procedure
plan a TAVR procedure
From the frontlines to the frontier: CT trends and innovations
November 06, 2018
by Lauren Dubinsky, Senior Reporter
Last year, market research publication Kalorama Information predicted the CT market, which was already valued at nearly $5 billion globally, would be the fastest growing segment among all medical imaging systems.
New scanners on the market are providing higher image quality with faster acquisition time, driving demand among cardiology and oncology departments. The systems are being packaged with new and improved applications to simplify the exam process and radiation dose optimization technology to ensure patients are being imaged in the safest and most efficient ways possible.
“Most partial CT scans take just seconds, and a full scan of the entire body can be completed in about a half hour,” said Bruce Carlson, publisher of Kalorama Information. “The CT scan can record images of bone, soft tissue and blood vessels simultaneously, offering advantages over standard X-rays.”
As artificial intelligence (AI) gains ground in the medical imaging sector, CT systems are poised to do more with less. For Carlson, the convergence of machine learning and CT is one of several AI-related topics he plans to examine more thoroughly in the coming year.
 “Due to the digital and representative ‘computed’ nature of CT – [the fact that it’s] not merely an image, but actually created from the imaging process – it lends itself to mathematical interpretation,” he said. “After all, it is created by math, so it's logical to think a computer could read it as well as an eye.”
“Due to the digital and representative ‘computed’ nature of CT – [the fact that it’s] not merely an image, but actually created from the imaging process – it lends itself to mathematical interpretation,” he said. “After all, it is created by math, so it's logical to think a computer could read it as well as an eye.”
Seeing results with AI
One company that has found early success forging inroads into AI with CT is Aidoc, an Israel-based startup that launched the world’s first AI-powered full-body solution for CT analysis in February. The tool is designed to help radiologists identify medically significant abnormalities throughout the body including the head, c-spine, chest and abdomen.
Unlike on-demand solutions that clinicians have to access through a separate interface, the Aidoc system is readily available to highlight urgent cases as they enter a clinician’s worklist.
“Our AI is always on in the background, ensuring that the radiologist gets the value directly in their work environment,” said Elad Walach, CEO of Aidoc. “It really enhances the radiologist's peace of mind knowing we are there for them.”
The Aidoc Full Body Solution has already been deployed in more than 50 hospitals worldwide. Two days after it was deployed at a university hospital in the U.S., Walach said it flagged a patient with an intracranial hemorrhage who needed urgent treatment.
“This patient would have been released home and only looked at the day after [because of] this site's workflow,” said Walach. “Instead, the radiologists were able to reach him on time, and make sure he gets admitted on the spot.”
Aidoc is not the only group doing work in this field. For example, a research team at Icahn School of Medicine at Mount Sinai in New York has developed AI software for CT that can identify stroke, hemorrhage and other neurological problems in 1.2 seconds. Another team at the University of Central Florida’s Computer Vision Research Center is developing an AI solution that can detect tiny masses of lung cancer in CT scans, and that’s just the tip of the iceberg.
 With all these computer algorithms poised to enhance the way scans are read, there has been a lot of talk about what this will mean for the role of radiologists in the future. Most experts agree that imaging providers should not worry about being displaced by AI, but need to become comfortable with the new technology so that it can serve them in their efforts to become more efficient.
With all these computer algorithms poised to enhance the way scans are read, there has been a lot of talk about what this will mean for the role of radiologists in the future. Most experts agree that imaging providers should not worry about being displaced by AI, but need to become comfortable with the new technology so that it can serve them in their efforts to become more efficient.
“Radiology is the most data-driven field in medicine and the majority of radiologists I speak to realize that AI solutions are here to help,” said Walach. “AI has the ability to sift through the growing piles of data and help radiologists make decisions faster and more accurately.”
One facility’s experience with LDCT lung cancer screening
With the American Cancer Society estimating that over 200,000 new cases of lung cancer will be diagnosed in the U.S. this year, low-dose CT scanning is vital for patients with a long history of smoking. Unfortunately, access and awareness can be lacking among the populations who need screening most.
The University of Michigan Medicine implemented its low-dose CT lung cancer screening program in the early 2000s, but it wasn’t until the past few years that it began to gain traction. The program is currently approaching approximately 100 patients per month.
In December 2013, the USPSTF recommended annual low-dose CT screening for lung cancer for patients 55 to 80 years old with a 30 pack-year smoking history, and who currently smoke or who quit in the last 15 years. CMS followed up with its decision to provide coverage for these exams in February 2015.
 “This has been very beneficial to this patient population,” said Dr. Ella Kazerooni, service chief of diagnostic radiology at University of Michigan Medicine. “This is the leading cause of cancer death in the U.S. and abroad, for which there has been no screening test.”
“This has been very beneficial to this patient population,” said Dr. Ella Kazerooni, service chief of diagnostic radiology at University of Michigan Medicine. “This is the leading cause of cancer death in the U.S. and abroad, for which there has been no screening test.”
She added that while many people are familiar with screening for breast and colon cancer, they are not always aware that there are similar services for detecting lung cancer.
When a patient is diagnosed with lung cancer, her department works closely with the pulmonary medicine department to ensure they are getting their follow-up CT scans at the three- or six-month mark. She noted that it’s important not to let any patient “fall through the cracks.”
Although Kazerooni stressed that the financial aspects of lung cancer screening are far less important than the medical appropriateness of the exams, she doesn’t think costs should prohibit other providers from implementing their own programs.
“If an institution were to look at the economics, they would find it to be very viable even after the investment in the supporting staff and technology that’s required,” she said. “I think they should not think of the economic side as an obstacle to their practice.”
For all the lifesaving value of low dose CT lung cancer screening, analysis shows that the scans have also been plagued by a high rate of false positives. In an effort to address this, Fox Chase Cancer Center in Philadelphia received a $673,000 grant from the U.S. Department of Defense in August to develop a test that detects early-stage lung cancer and can serve as a secondary screening option for patients with inconclusive lung CT scans.
Fox Chase and the Philadelphia VA Medical Center are planning on enrolling patients in a study later this year to evaluate the efficacy of the new test.
Breast CT… without radiation?
Although CT and radiation are commonly thought to go hand-in-hand, Lihong Wang, professor of medical and electrical engineering at The California Institute of Technology (Caltech), doesn’t believe computed tomography has to be thought of in that way.
He and his research team at Caltech have developed a laser-sonic scanner that utilizes photoacoustic CT (PACT) to locate breast cancer tumors in as little as 15 seconds without the need for radiation dose exposure.
PACT uses two forms of energy – light and sound. A light pulse that is fired into the tissue is converted to sound inside the tissue and the clinician listens to the sound outside of the tissue.
“We are combining the advantages of both light and sound for imaging,” said Wang. “Both are entirely safe to humans, unlike X-ray, which can cause DNA damage.”
In addition, PACT shows molecular information, which is something X-ray-based CT cannot do.
 A prototype is currently under development by a Pasadena-based company called CalPACT. For an idea of what this system will ultimately look like, Wang described a bed with a hole in the middle.
A prototype is currently under development by a Pasadena-based company called CalPACT. For an idea of what this system will ultimately look like, Wang described a bed with a hole in the middle.
The patient will lie face down on the table with one breast at a time placed in a recess that contains 512 tiny ultrasonic sensors. A near-infrared laser light pulse will be shot from underneath the breast, diffuse through the tissue and be absorbed by oxygen-carrying hemoglobin molecules into the patient’s red blood cells.
Wang and his team tested the technology in a pilot study and it identified eight of the nine tumors that were present in the breasts of the eight study participants.
When asked if he thinks PACT could eventually replace mammography as the standard screening modality for breast cancer, he said that he “certainly hopes so.” Although he acknowledges that mammography is relatively fast, effective and affordable, he points to the use of ionizing radiation, a high false positive rate, and difficulty imaging young women as areas where new technology may someday offer advantages.
“My hope is that we can do far better than that,” said Wang. “Even though the initial investment will be higher because our system will be more expensive than a standard mammography system, the benefit will be far greater.”
For now, PACT is being investigated strictly for detecting breast cancer, but Wang and his team are looking at diabetic foot, neonatal brain imaging, whole-body neonatal imaging, standard extremity imaging and even adult human brain imaging as other potential applications for the imaging technology.
“Adult brain imaging is the toughest because we have to deal with the thick human skull,” said Lihong. “Ultrasound waves come out with pretty strong distortion due to the skull, so we are working on all sorts of methods to conquer that problem.”
CT is climbing off the screen
With sophisticated 3D printing technology, radiologists are now able to see the imaged anatomy in an actual 3D model replica they can hold in their hand.
 “For some procedures that would be overkill and wouldn’t be necessary, but for other procedures surgeons find it helpful, particularly in complex cases like congenital heart disease,” said Dr. Gary Danton, vice chair of education and program director of radiology residency at Jackson Memorial Hospital in Miami.
“For some procedures that would be overkill and wouldn’t be necessary, but for other procedures surgeons find it helpful, particularly in complex cases like congenital heart disease,” said Dr. Gary Danton, vice chair of education and program director of radiology residency at Jackson Memorial Hospital in Miami.
His hospital uses Canon CT systems to generate images of the heart that are used to 3D print the models for surgical planning.
“There are different ways to do it – we do have a surgeon who is doing in-house 3D printing on a case-by-case basis, and there are companies you can send data to and have 3D-printed models made,” Danton explained.
Unfortunately, he added, this technology can be expensive, and since there is currently not an easy way to get reimbursed for this kind of work, it’s something that is done sparingly.
There are many costs associated with making these models, including the cost of the printer, the person running the printer, the materials, as well as the time it takes to design the model. You can’t simply take data from the CT, hit print and have a model pop out – a well-trained person needs to perform a lot of preparation and reconstruction work.
 “If the government or payors are going to pay for something, they want to know that it actually adds value and it’s not just fun and exciting,” said Danton. “It actually has to have better outcomes associated with it.”
“If the government or payors are going to pay for something, they want to know that it actually adds value and it’s not just fun and exciting,” said Danton. “It actually has to have better outcomes associated with it.”
Better outcomes can come in many different forms. It could mean that the models allow the surgeons to perform the procedure less invasively, they reduce OR time since the surgeons can figure something out before they begin the procedure or they improve the surgeons’ confidence.
“It may be difficult to come up with a particular outcome measure that demonstrates the utility, but it doesn’t mean there aren’t benefits and that it’s not useful,” said Danton. “It just may be hard to measure.”
Many studies are currently underway to investigate this, but it may be a while before meaningful results are published.
“My guess would be that for some procedures, it’s going to be very useful and for others maybe not so much, but figuring that out will take some time,” Danton concluded.
EDIT: An earlier version of this article incorrectly stated that the Caltech laser-sonic scanner could locate breast cancer tumors in "15 minutes" — we have updated the article to indicate that it can locate the cancer within 15 seconds.
New scanners on the market are providing higher image quality with faster acquisition time, driving demand among cardiology and oncology departments. The systems are being packaged with new and improved applications to simplify the exam process and radiation dose optimization technology to ensure patients are being imaged in the safest and most efficient ways possible.
“Most partial CT scans take just seconds, and a full scan of the entire body can be completed in about a half hour,” said Bruce Carlson, publisher of Kalorama Information. “The CT scan can record images of bone, soft tissue and blood vessels simultaneously, offering advantages over standard X-rays.”
As artificial intelligence (AI) gains ground in the medical imaging sector, CT systems are poised to do more with less. For Carlson, the convergence of machine learning and CT is one of several AI-related topics he plans to examine more thoroughly in the coming year.

Bruce Carlson
Seeing results with AI
One company that has found early success forging inroads into AI with CT is Aidoc, an Israel-based startup that launched the world’s first AI-powered full-body solution for CT analysis in February. The tool is designed to help radiologists identify medically significant abnormalities throughout the body including the head, c-spine, chest and abdomen.
Unlike on-demand solutions that clinicians have to access through a separate interface, the Aidoc system is readily available to highlight urgent cases as they enter a clinician’s worklist.
“Our AI is always on in the background, ensuring that the radiologist gets the value directly in their work environment,” said Elad Walach, CEO of Aidoc. “It really enhances the radiologist's peace of mind knowing we are there for them.”
The Aidoc Full Body Solution has already been deployed in more than 50 hospitals worldwide. Two days after it was deployed at a university hospital in the U.S., Walach said it flagged a patient with an intracranial hemorrhage who needed urgent treatment.
“This patient would have been released home and only looked at the day after [because of] this site's workflow,” said Walach. “Instead, the radiologists were able to reach him on time, and make sure he gets admitted on the spot.”
Aidoc is not the only group doing work in this field. For example, a research team at Icahn School of Medicine at Mount Sinai in New York has developed AI software for CT that can identify stroke, hemorrhage and other neurological problems in 1.2 seconds. Another team at the University of Central Florida’s Computer Vision Research Center is developing an AI solution that can detect tiny masses of lung cancer in CT scans, and that’s just the tip of the iceberg.
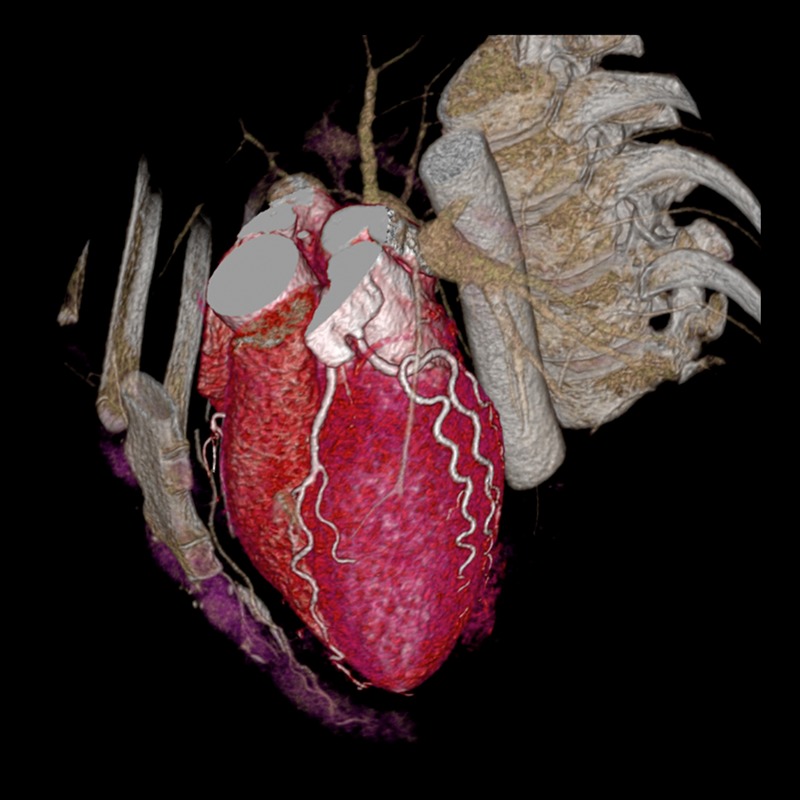
CT scan generated with a Canon
CT to plan a TAVR procedure
CT to plan a TAVR procedure
“Radiology is the most data-driven field in medicine and the majority of radiologists I speak to realize that AI solutions are here to help,” said Walach. “AI has the ability to sift through the growing piles of data and help radiologists make decisions faster and more accurately.”
One facility’s experience with LDCT lung cancer screening
With the American Cancer Society estimating that over 200,000 new cases of lung cancer will be diagnosed in the U.S. this year, low-dose CT scanning is vital for patients with a long history of smoking. Unfortunately, access and awareness can be lacking among the populations who need screening most.
The University of Michigan Medicine implemented its low-dose CT lung cancer screening program in the early 2000s, but it wasn’t until the past few years that it began to gain traction. The program is currently approaching approximately 100 patients per month.
In December 2013, the USPSTF recommended annual low-dose CT screening for lung cancer for patients 55 to 80 years old with a 30 pack-year smoking history, and who currently smoke or who quit in the last 15 years. CMS followed up with its decision to provide coverage for these exams in February 2015.
Dr. Ella Kazerooni
She added that while many people are familiar with screening for breast and colon cancer, they are not always aware that there are similar services for detecting lung cancer.
When a patient is diagnosed with lung cancer, her department works closely with the pulmonary medicine department to ensure they are getting their follow-up CT scans at the three- or six-month mark. She noted that it’s important not to let any patient “fall through the cracks.”
Although Kazerooni stressed that the financial aspects of lung cancer screening are far less important than the medical appropriateness of the exams, she doesn’t think costs should prohibit other providers from implementing their own programs.
“If an institution were to look at the economics, they would find it to be very viable even after the investment in the supporting staff and technology that’s required,” she said. “I think they should not think of the economic side as an obstacle to their practice.”
For all the lifesaving value of low dose CT lung cancer screening, analysis shows that the scans have also been plagued by a high rate of false positives. In an effort to address this, Fox Chase Cancer Center in Philadelphia received a $673,000 grant from the U.S. Department of Defense in August to develop a test that detects early-stage lung cancer and can serve as a secondary screening option for patients with inconclusive lung CT scans.
Fox Chase and the Philadelphia VA Medical Center are planning on enrolling patients in a study later this year to evaluate the efficacy of the new test.
Breast CT… without radiation?
Although CT and radiation are commonly thought to go hand-in-hand, Lihong Wang, professor of medical and electrical engineering at The California Institute of Technology (Caltech), doesn’t believe computed tomography has to be thought of in that way.
He and his research team at Caltech have developed a laser-sonic scanner that utilizes photoacoustic CT (PACT) to locate breast cancer tumors in as little as 15 seconds without the need for radiation dose exposure.
PACT uses two forms of energy – light and sound. A light pulse that is fired into the tissue is converted to sound inside the tissue and the clinician listens to the sound outside of the tissue.
“We are combining the advantages of both light and sound for imaging,” said Wang. “Both are entirely safe to humans, unlike X-ray, which can cause DNA damage.”
In addition, PACT shows molecular information, which is something X-ray-based CT cannot do.

Lihong Wang
The patient will lie face down on the table with one breast at a time placed in a recess that contains 512 tiny ultrasonic sensors. A near-infrared laser light pulse will be shot from underneath the breast, diffuse through the tissue and be absorbed by oxygen-carrying hemoglobin molecules into the patient’s red blood cells.
Wang and his team tested the technology in a pilot study and it identified eight of the nine tumors that were present in the breasts of the eight study participants.
When asked if he thinks PACT could eventually replace mammography as the standard screening modality for breast cancer, he said that he “certainly hopes so.” Although he acknowledges that mammography is relatively fast, effective and affordable, he points to the use of ionizing radiation, a high false positive rate, and difficulty imaging young women as areas where new technology may someday offer advantages.
“My hope is that we can do far better than that,” said Wang. “Even though the initial investment will be higher because our system will be more expensive than a standard mammography system, the benefit will be far greater.”
For now, PACT is being investigated strictly for detecting breast cancer, but Wang and his team are looking at diabetic foot, neonatal brain imaging, whole-body neonatal imaging, standard extremity imaging and even adult human brain imaging as other potential applications for the imaging technology.
“Adult brain imaging is the toughest because we have to deal with the thick human skull,” said Lihong. “Ultrasound waves come out with pretty strong distortion due to the skull, so we are working on all sorts of methods to conquer that problem.”
CT is climbing off the screen
With sophisticated 3D printing technology, radiologists are now able to see the imaged anatomy in an actual 3D model replica they can hold in their hand.

Dr. Gary Danton
His hospital uses Canon CT systems to generate images of the heart that are used to 3D print the models for surgical planning.
“There are different ways to do it – we do have a surgeon who is doing in-house 3D printing on a case-by-case basis, and there are companies you can send data to and have 3D-printed models made,” Danton explained.
Unfortunately, he added, this technology can be expensive, and since there is currently not an easy way to get reimbursed for this kind of work, it’s something that is done sparingly.
There are many costs associated with making these models, including the cost of the printer, the person running the printer, the materials, as well as the time it takes to design the model. You can’t simply take data from the CT, hit print and have a model pop out – a well-trained person needs to perform a lot of preparation and reconstruction work.

Single Breath Hold PACT
Better outcomes can come in many different forms. It could mean that the models allow the surgeons to perform the procedure less invasively, they reduce OR time since the surgeons can figure something out before they begin the procedure or they improve the surgeons’ confidence.
“It may be difficult to come up with a particular outcome measure that demonstrates the utility, but it doesn’t mean there aren’t benefits and that it’s not useful,” said Danton. “It just may be hard to measure.”
Many studies are currently underway to investigate this, but it may be a while before meaningful results are published.
“My guess would be that for some procedures, it’s going to be very useful and for others maybe not so much, but figuring that out will take some time,” Danton concluded.
EDIT: An earlier version of this article incorrectly stated that the Caltech laser-sonic scanner could locate breast cancer tumors in "15 minutes" — we have updated the article to indicate that it can locate the cancer within 15 seconds.